


30 Jul Plantar Heel Pain Notes
Is a generalised term to describe a range of undifferentiated conditions affecting the plantar heel.1
Recent imaging techniques are showing the condition actually affects more than just the plantar fascia (e.g. heel bone and surrounding tissue) and the more generalised term, plantar heel pain, is indicated as being more appropriate.2
Plantar fasciitis is reported as the most common cause of CPHP.
It is important to note that similar to damage to tendons it has been shown it is not an inflammation of the plantar fascia but more a degenerative pathology.3 The term fasciopathy is therefore more appropriate to describe the condition.3
Note: plantar fasciitis and plantar fasciopathy will be used interchangeably throughout as appropriated used in the citations.
Differential diagnoses to consider include calcaneal fracture, heel pad atrophy and pain of neural origin.4
CPHP can also be associated with inflammation conditions such as spondyloarthrosis1 and an important consideration when taking a patient’s history.
Epidemiology
Reliable population based incidence data is lacking in many countries.4
An Australian population based study involving 3206 randomly selected participants has reported a heel pain prevalence of 3.6%1
American studies estimate that 7% of older adults report tenderness beneath the heel, and that 1 million physician consultations per year are for the diagnosis and treatment of plantar fasciitis.1
In relation to the diagnosis of plantar fasciitis in recreational runners the incidence has been reported at approximately 5%, after medial tibial stress syndrome (10%), patella-femoral pain (10%), medial meniscus injury (9%), and Achilles tendinopathy (7%).3
Plantar Fasciopathy/Fasciitis
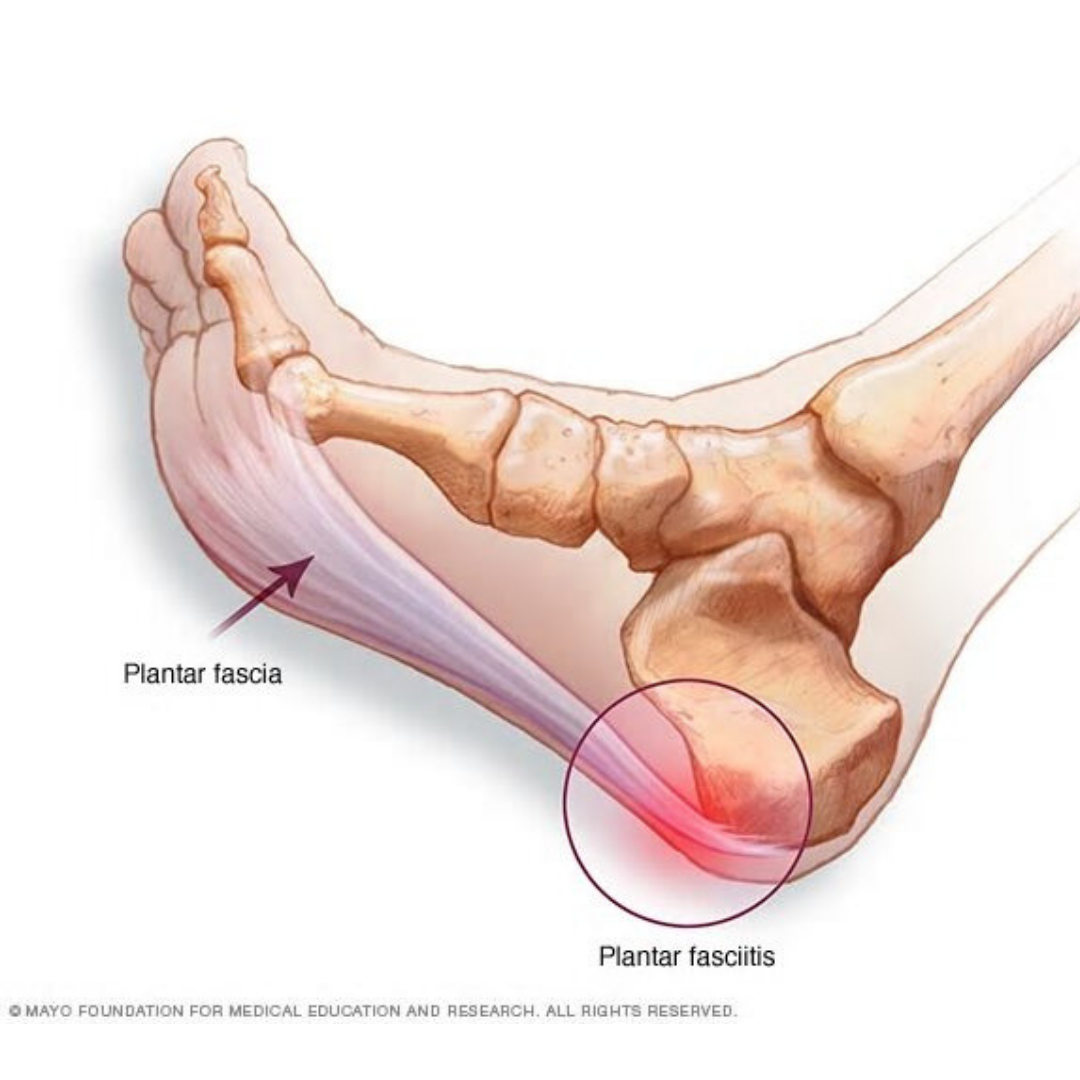
Anatomy of the Plantar Fascia
The plantar fascia is a thick sheath of type 1 collagen that supports the arch of the foot.5
The plantar fascia starts proximally at the calcaneus and extends distally into five separate bands that become the digital sheaths.6
These bands radiate towards and attach through the plantar plate to the proximal phalanges.7
It has a medial, lateral and central part with the central part also known as the plantar aponeurosis. This thickest central part of the plantar fascia is of particular importance as it plays an important functional role of supporting the medial longitudinal arch of the foot during weight bearing as well as lifting the arch during movement.
Together with the bones of the arch of the foot it forms a triangular truss which helps prevent the arch from separating and collapsing.7
During bending of the toes during both walking and running a mechanism called the Windlass mechanism causes the plantar aponeurosis to tighten contributing to the raising of the medial longitudinal arch.7
Symptoms
Typified by pain first thing in the morning and/or after getting up from long periods of rest.
This can then ease off but then return after being on your feet for extended periods of walking, standing or after an intense exercise or running session.
Aetiology & Risk Factors of Plantar Fasciitis
The causes are not fully understood but the suggested risk factors for the general population include being overweight, older age, prolonged standing, and having reduced range of motion in the ankle and 1st metatarsal-phalangeal joint. A pronated foot posture has been linked with the condition, but it has not been consistently found to be a risk factor.2
Running – Petralglia et al. (2017) identified risk factors for running and has broken it into intrinsic (anatomical, functional and degenerative) and extrinsic (overuse, in-correct training and inadequate footwear) risk factors. Specific levels of evidence have been given for each of the specific points listed below but nonetheless they are in line with what are commonly identified by health practitioners including Podiatrists and should be at least considered and therefore addressed when looking at the whole runner’s injury picture.
Intrinsic
Anatomical – Pes Planus (low or flat arches), Pes Cavus (very high arches), Overpronation, Leg length difference, excessive lateral tibial torsion, excessive femoral anteversion, overweight.3
Functional – Gastrocnemius & Soleus muscle (calf muscle) tightness, Achilles tendon tightness, calf and instrinsic foot muscle weakness.3
Degenerative – Aging of the fat pad, atrophy of the heel fat pad, plantar fascia stiffness.3
Extrinsic
Overuse – Mechanical stresses and tearing.3
Incorrect training (training error) – A too fast increase in the distance, intensity, duration or frequency of activities that involve repetitive loading of the feet.3
Inadequate footwear – Poorly cushioned surface, inappropriate replacement of worn out shoes.3
Histopathology
Increased mucoid ground substance, collagen degeneration and angiofibroblastic hyperplasia.1
Markers of persistent inflammation such as lymphocyte and macrophage infiltration have been less frequently reported in the condition.1
Plantar fasciitis may follow a similar pathological pathway to that of tendinopathy where tissue changes are thought to proceed from an early reactive phase to progressive degeneration.1
Pathomechanics
The development of plantar fasciitis has traditionally thought to have a mechanical origin.
In particular pes planus foot types and lower-limb biomechanics that result in a lowered medial longitudinal arch have been thought to create excessive tensile strain within the fascia, producing microscopic tears and chronic inflammation.
However histological evidence does not support this concept, with inflammation rarely observed in chronic plantar fasciitis.8
Similarly scientific support for the role of arch mechanics in the development of plantar fasciitis is equivocal, despite an abundance of anecdotal evidence indicating a causal link between arch function and heel pain.9
This may, in part, reflect the difficulty in measuring arch mechanics in vivo.9
However, it may also indicate that tensile failure is not a predominant feature in the pathomechanics of plantar fasciitis.8
Alternative mechanisms including ‘stress-shielding’, vascular and metabolic disturbances, the formation of free radicals, hyperthermia and genetic factors have also been linked to degenerative change in connective tissues.8
Imaging
Useful especially if the condition does not respond to conservative first line interventions or when considering more invasive treatments.1
MRI, Ultrasound and X- ray
Ultrasound useful – greater than 4mm considered diagnostic of plantar fasciitis.1
Xray – Presence of heel spurs
Uncertainty as there is a high prevalence of subcalcaneal spurs in asymptomatic population.1
Still there is a strong association with pain beneath the heel.1
The location of the heel spur actually occurs deep to the plantar fascia insertion closely associated with abductor hallucis and flexor digitorum brevis origins
Formation has been traditionally associated with repetitive longitudinal traction of the plantar fascia. It is suggested however that vertical compressive forces may play a more important role.1
Treatment
While symptoms typically improve within a year of onset regardless of treatment, approximately 40% of patients continue to have symptoms after 2 years.5
Summary of treatment – Limited evidence for clear effective treatment path
Landorf systematic overview 2015

*Image Reference 10
Principal treatment strategies for management of plantar fasciitis – Petralglia et al. (2017)3

Not mentioned above yet commonly implemented…..
High-load strength training – suggested similar to effect this has on tendons – high load training may aide in a quicker reduction in pain and improvements in function.11
One option to induce controlled high-load tensile forces across the plantar fascia is by the combined use of Achilles tendon loading and the windlass mechanism.11
The windlass mechanism causes tightening of the plantar fascia during dorsal flexion of the metatarsophalangeal joints.11
Additionally, the close anatomical connection between the Achilles tendon, paratendon, and the plantar fascia suggests that high loading of the Achilles tendon is transferred to the plantar fascia.11
Rathleff et al.11 concluded in their RCT that a simple progressive exercise protocol consisting of high-load strength training, performed every second day, resulted in a superior outcome at 3 months compared with plantar-specific stretching and may aid in a quicker reduction in pain and improvements in function. However, there were no significant benefits of high-load strength training at the secondary endpoints at 1, 6, and 12 months. This study adds new evidence for the positive effect of a simple, progressive exercise protocol for a severe and debilitating condition.
Podiatry Intervention complimentary to Physical therapy treatment
Primarily aimed at attempting to deload the plantar fascia and provide impact comfort
Taping – low dye that is specific for foot and flexibility type
Padding – Rearfoot VR & Forefoot VL padding – aimed at complimenting taping or replacing if can not use tape
Heel raises – to address ankle equinus – complement taping and padding
Off the shelf &/or custom orthotics – if need a longer term solution for chronic cases to achieve similar results to padding and taping.
Footwear management – 10mm heel raise built into traditional running shoes – working at convincing patient of need, working on work and casual options
Straussberg sock – when to implement?
Shockwave – when to implement?
CAM walker – when all else is failing – 2/3 weeks max?
Descision on imaging – xray vs ultrasound vs MRI?
Referral to Sport Physician – when all else fails – they usually want to know that all aspects have been ticked off in terms of attempting to deload, can use PRP via ultrasound guided injection?

REFERENCE LIST
1 MCMILLAN, A. M. et al. Diagnostic imaging for chronic plantar heel pain: a systematic review and meta-analysis. J Foot Ankle Res, v. 2, p. 32, Nov 2009. ISSN 1757-1146. Disponível em: < https://www.ncbi.nlm.nih.gov/pubmed/19912628 >.
2 LANDORF, K. B. Plantar heel pain and plantar fasciitis. BMJ Clin Evid, v. 2015, Nov 2015. ISSN 1752-8526. Disponível em: < https://www.ncbi.nlm.nih.gov/pubmed/26609884 >.
3 PETRAGLIA, F.; RAMAZZINA, I.; COSTANTINO, C. Plantar fasciitis in athletes: diagnostic and treatment strategies. A systematic review. Muscles Ligaments Tendons J, v. 7, n. 1, p. 107-118, 2017 Jan-Mar 2017. ISSN 2240-4554. Disponível em: < https://www.ncbi.nlm.nih.gov/pubmed/28717618 >.
4 SWEETING, D. et al. The effectiveness of manual stretching in the treatment of plantar heel pain: a systematic review. J Foot Ankle Res, v. 4, p. 19, Jun 2011. ISSN 1757-1146. Disponível em: < https://www.ncbi.nlm.nih.gov/pubmed/21703003 >.
5 DIGIOVANNI, B. F. et al. Plantar fascia-specific stretching exercise improves outcomes in patients with chronic plantar fasciitis. A prospective clinical trial with two-year follow-up. J Bone Joint Surg Am, v. 88, n. 8, p. 1775-81, Aug 2006. ISSN 0021-9355. Disponível em: < https://www.ncbi.nlm.nih.gov/pubmed/16882901 >.
6 BOURNE, M.; VARACALLO, M. Anatomy, Bony Pelvis and Lower Limb, Foot Fascia. In: (Ed.). StatPearls. Treasure Island (FL): StatPearls Publishing. StatPearls Publishing LLC., 2018.
7 CHEN, D. W. et al. Anatomy and biomechanical properties of the plantar aponeurosis: a cadaveric study. PLoS One, v. 9, n. 1, p. e84347, 2014. ISSN 1932-6203. Disponível em: < https://www.ncbi.nlm.nih.gov/pubmed/24392127 >.
8 DE CLERCQ, D. L. Ankle bracing in running: the effect of a Push type medium ankle brace upon movements of the foot and ankle during the stance phase. Int J Sports Med, v. 18, n. 3, p. 222-8, Apr 1997. ISSN 0172-4622. Disponível em: < https://www.ncbi.nlm.nih.gov/pubmed/9187979 >.
9 WEARING, S. C. et al. The pathomechanics of plantar fasciitis. Sports Med, v. 36, n. 7, p. 585-611, 2006. ISSN 0112-1642. Disponível em: < https://www.ncbi.nlm.nih.gov/pubmed/16796396 >.
10 LANDORF, K. B.; MENZ, H. B. Plantar heel pain and fasciitis. BMJ Clin Evid, v. 2008, Feb 2008. ISSN 1752-8526. Disponível em: < https://www.ncbi.nlm.nih.gov/pubmed/19450330 >.
11 RATHLEFF, M. S. et al. High-load strength training improves outcome in patients with plantar fasciitis: A randomized controlled trial with 12-month follow-up. Scand J Med Sci Sports, v. 25, n. 3, p. e292-300, Jun 2015. ISSN 1600-0838. Disponível em: < https://www.ncbi.nlm.nih.gov/pubmed/25145882 >.
No Comments